Abstract
Mechanically ventilated patients with acute respiratory distress syndrome (ARDS) often receive aerosolized iloprost. Due to the short half-life of prostacyclin, extending the duration of inhalation could enhance its clinical effectiveness, though this presents technical difficulties. One potential solution is the use of inspiration-synchronized vibrating mesh nebulizers (VMNsyn), which offer high drug deposition rates and prolonged nebulization times. However, there is a lack of data comparing prolonged nebulization with bolus delivery of iloprost using continuous vibrating mesh nebulizers (VMNcont), as well as examining the impact of different ventilation modes on inspiration-synchronized nebulization. To address this gap, an in vitro study was conducted using a mechanical ventilation model for adults, comparing the VMNsyn and VMNcont in both volume-controlled (VC-CMV) and pressure-controlled continuous mandatory ventilation (PC-CMV) modes. The study assessed the iloprost deposition rate and nebulization time. In VC-CMV mode, the deposition rate of the VMNsyn was similar to that of the VMNcont, but 10.9% lower in PC-CMV mode. The aerosol output from the VMNsyn was significantly lower than that of the VMNcont in both modes, resulting in a 7.5-fold longer nebulization time in VC-CMV and a 4.2-fold longer time in PC-CMV. Thus, inspiration-synchronized nebulization in VC-CMV mode appears to be the most effective method for prolonged inhalation of iloprost in mechanically ventilated patients.
Introduction
Acute respiratory distress syndrome (ARDS) is characterized by pulmonary vascular dysfunction, which leads to acute pulmonary hypertension, progressive right heart failure, and the development of acute cor pulmonale . A variety of drugs are available for treating acute right heart failure, many of which are repurposed from the management of primary pulmonary hypertension (PPH) and are typically administered either orally or intravenously. However, systemic administration often lacks pulmonary selectivity, leading to side effects such as generalized vasodilation and pulmonary vasodilation in non-ventilated lung areas, which can worsen hypoxemia . Pulmonary delivery of drugs can help mitigate these adverse effects, as demonstrated with the prostacyclin analogue iloprost.
In ARDS patients, nebulization of 5 µg of iloprost has been shown to improve oxygenation without significantly lowering systemic blood pressure. However, no studies have yet proven that such interventions improve patient outcomes . One possible explanation is that in these studies, iloprost was administered via continuous nebulization ], delivering a large bolus of the drug over a short period of time. Given that the half-life of iloprost ranges from several minutes to a maximum of 30 minutes, the therapeutic effect may diminish quickly after administration. To address this, prolonged intravenous infusion regimens of iloprost have been investigated in patients with severe PPH. To avoid systemic vasodilation in the often hemodynamically unstable ARDS patients, a prolonged inhalation regimen would be more preferable. However, this approach has not been clinically evaluated, likely due to the technical challenges associated with prolonged inhaled aerosol administration in routine clinical practice
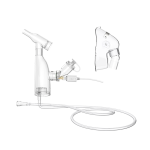
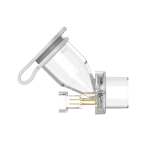
A practical solution to this issue could be the use of inspiration-synchronized vibrating mesh nebulizers (VMNsyn), which are already employed for aerosolizing antibiotics in mechanically ventilated patients. By synchronizing aerosol delivery with the inspiratory airflow, VMNsyn can achieve nebulization times that are three to nine times longer than bolus delivery, while maintaining similar or even higher drug deposition rates due to reduced drug loss during exhalation.
Therefore, in an in vitro model of mechanically ventilated adults, the drug deposition rate and the nebulization time of an inspiration-synchronized vibrating mesh nebulizer (VMNsyn) and a continuous vibrating mesh nebulizer (VMNcont) were compared in two basic ventilation modes: (A) volume-controlled continuous mandatory ventilation (VC-CMV) and (B) pressure-controlled continuous mandatory ventilation (PC-CMV).
Results and Conclusion
In this in vitro model of a mechanically ventilated patient, a conventional inspiration-synchronized vibrating mesh nebulizer (VMNsyn) used in the VC-CMV mode achieved iloprost deposition rates similar to those obtained with bolus administration using a continuous nebulizer (VMNcont), while also demonstrating a 7.5-fold longer nebulization time. This setup appears suitable for the prolonged inhalation of iloprost in mechanically ventilated patients.
However, in the PC-CMV mode, the VMNsyn’s deposition rate was significantly lower, and the nebulization time was notably reduced, undermining the intended prolonged drug administration and minimizing the potential benefits of iloprost. Therefore, future development of commercial VMNsyn models should focus on optimizing aerosol release during the initial phase of inspiration. This would allow the deposition rate and nebulization time to become less dependent on the ventilation mode, enabling the VMNsyn to maximize its drug-saving potential and achieve even higher deposition rates than the VMNcont.
Nevertheless, the impact of prolonged inhalative iloprost administration with a VMNsyn on pharmacokinetics and therapeutic outcomes still requires investigation in clinical trials. A randomized cross-over study in mechanically ventilated ARDS patients could provide valuable insights into the effects of prolonged pulmonary iloprost administration on pharmacokinetics, pulmonary vascular resistance, right heart function, oxygenation, and hemodynamics, compared to bolus nebulization.
Refernence
[1]Price, L.C.; McAuley, D.F.; Marino, P.S.; Finney, S.J.; Griffiths, M.J.; Wort, S.J. Pathophysiology of pulmonary hypertension in acute lung injury. Am. J. Physiol. Lung Cell Mol. Physiol. 2012, 302, L803–L815.
[2]Bull, T.M.; Clark, B.; McFann, K.; Moss, M. Pulmonary vascular dysfunction is associated with poor outcomes in patients with acute lung injury. Am. J. Respir. Crit. Care Med. 2010, 182, 1123–1128.
[3]Mekontso Dessap, A.; Boissier, F.; Charron, C.; Bégot, E.; Repessé, X.; Legras, A.; Brun-Buisson, C.; Vignon, P.; Vieillard-Baron, A. Acute cor pulmonale during protective ventilation for acute respiratory distress syndrome: Prevalence, predictors, and clinical impact. Intensive Care Med. 2016, 42, 862–870.
[4]Ganeriwal, S.; Alves dos Anjos, G.; Schleicher, M.; Hockstein, M.A.; Tonelli, A.R.; Duggal, A.; Siuba, M.T. Right ventricle-specific therapies in acute respiratory distress syndrome: A scoping review. Crit. Care 2023, 27, 104.
[5]Ymeraj, S.; Attou, R.; Redant, S. Right ventricule-specific therapies in ARDS: Other vasodilating agents to be considered. Crit. Care 2023, 27, 133.

中国大陆
简体中文
United Kingdom
English