Due to the characteristics of the lung tissue itself, the speed of lung absorption is very fast, no less than intravenous injection, such as isoproterenol aerosol can play a role in asthma 1-2min after inhalation.
The lungs are composed of trachea, bronchi, bronchioles, alveolar ducts and alveolar sacs. The number of alveolar sacs is estimated to reach 3-400 million, and the total surface area can reach 70-100㎡, which is 25 times the body surface area.
The alveolar wall is composed of a single layer of epithelial cells.
These alveolar cells are close to a dense capillary network (the total surface area of capillaries is about 90 square meters, and the blood flow is large). The thickness of the cell wall or capillary wall is only 0.5-1m, so the alveolar sacs are where gas and blood rapidly diffuse and exchange. The drug reaches the alveolar sac and is quickly absorbed and effective.
Particle size is the main factor affecting lung deposition performance. Particle size significantly affects the location and distribution of inhaled particles deposited in the lungs.
1. William Glover and others found through radioactive isotope tracing method that the deposition amount and distribution of drug particles in the lungs depend on the particle size.
2. Omars. Usmani et al.’s research on targeting local respiratory tract through inhalation administration found that after inhalation administration, the smaller the particle size, the greater the amount of drug particles deposited in the lungs, the deeper the reach, and the wider the deposition range.
3. Zanen, Rees et al. studied the clinical effects of three different particle size ranges (< 1μm, 2-5μm and 5-10μm), as shown in the figure:
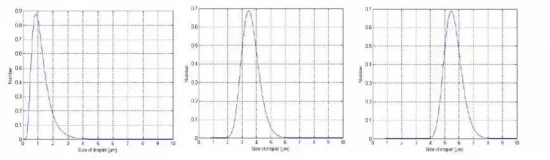
Through the above research data, we found that for drugs to be atomized into the lungs, the particle size should preferably be 2~5 μm. Particles with a size of 5 to 10 μm are mainly deposited in the oropharynx; particles with a size of 2 to 5 μm are mainly deposited in the lungs and bronchi, and 50% to 60% are deposited in the alveoli; particles that are too small (< 1 μm) are only It can reach the edge of the deep lungs and will be exhaled with breathing, so it has no therapeutic effect.
1. It must have a certain degree of hydrophilicity
It is best to dissolve in the secretions of the respiratory tract, otherwise it will become a foreign body and cause irritation to the respiratory tract.
2. It must have a certain lipophilicity
Substances are absorbed from the lungs by passive diffusion, and the absorption rate is related to the molecular weight and lipid solubility of the drug. Fat-soluble drugs are diffusely absorbed through the lipid bimolecular membrane, and a small part is absorbed through the small pores. Therefore, drugs with a large oil/water distribution coefficient are also absorbed quickly.
1. Non-atomized dosage forms can be used as atomized preparations
Drugs in non-aerosolized preparations cannot meet the requirements of aerosolized particles and cannot be cleared through the respiratory tract. They may be deposited in the lungs, thereby increasing the incidence of pulmonary infection. Atomized use is not recommended.
Common intravenous preparations contain preservatives (such as phenols, nitrites, etc.), which can induce asthma attacks after inhalation (excipients contained in non-inhaled drugs can irritate the respiratory tract).
2. Common injections that are not suitable for aerosol treatment
Dexamethasone injection: low fat solubility, high water solubility, little combination with airway mucosal tissue; large particle size, low lung deposition rate;
Gentamicin injection: The concentration of airway drugs is too low to achieve the purpose of anti-infection. The bacteria are in a sub-bacteriostatic state for a long time and develop drug resistance. At the same time, it can stimulate the airway epithelium and aggravate the epithelial inflammatory reaction;
Alpha-chymotrypsin injection: highly toxic to the retina, and can easily cause damage when in contact with the eyes when atomized; it is rapidly inactivated when exposed to blood and cannot be used for patients undergoing pharyngeal or lung surgery; it has been reported that this drug can damage lung tissue and inhale people's breath. It can aggravate inflammation and induce asthma in the tract;
Ambroxol Injection: Contains preservatives, which may induce bronchial asthma attacks after inhalation.
References:
"Expert Consensus on the Application of Nebulized Inhalation Therapy in Respiratory Diseases" Respiratory Disease Branch of the Chinese Medical Association
"Expert Consensus on Rational Use of Drugs in Nebulized Inhalation Therapy (2019 Edition)" Clinical Pharmacy Branch of the Chinese Medical Association
Rau JL. Respir Care, 2005, 50(3):,367-82.
Pitcairn G, et al. J Aerosol Med. 2005;18:264-272
Clover W, Chan HK Effect of particle size of dry powder mannitol on the lung deposition in health 2008,349(1/2):314-322

中国大陆
简体中文
United Kingdom
English